
Day 1 - Ischemic Stroke
Assessment:
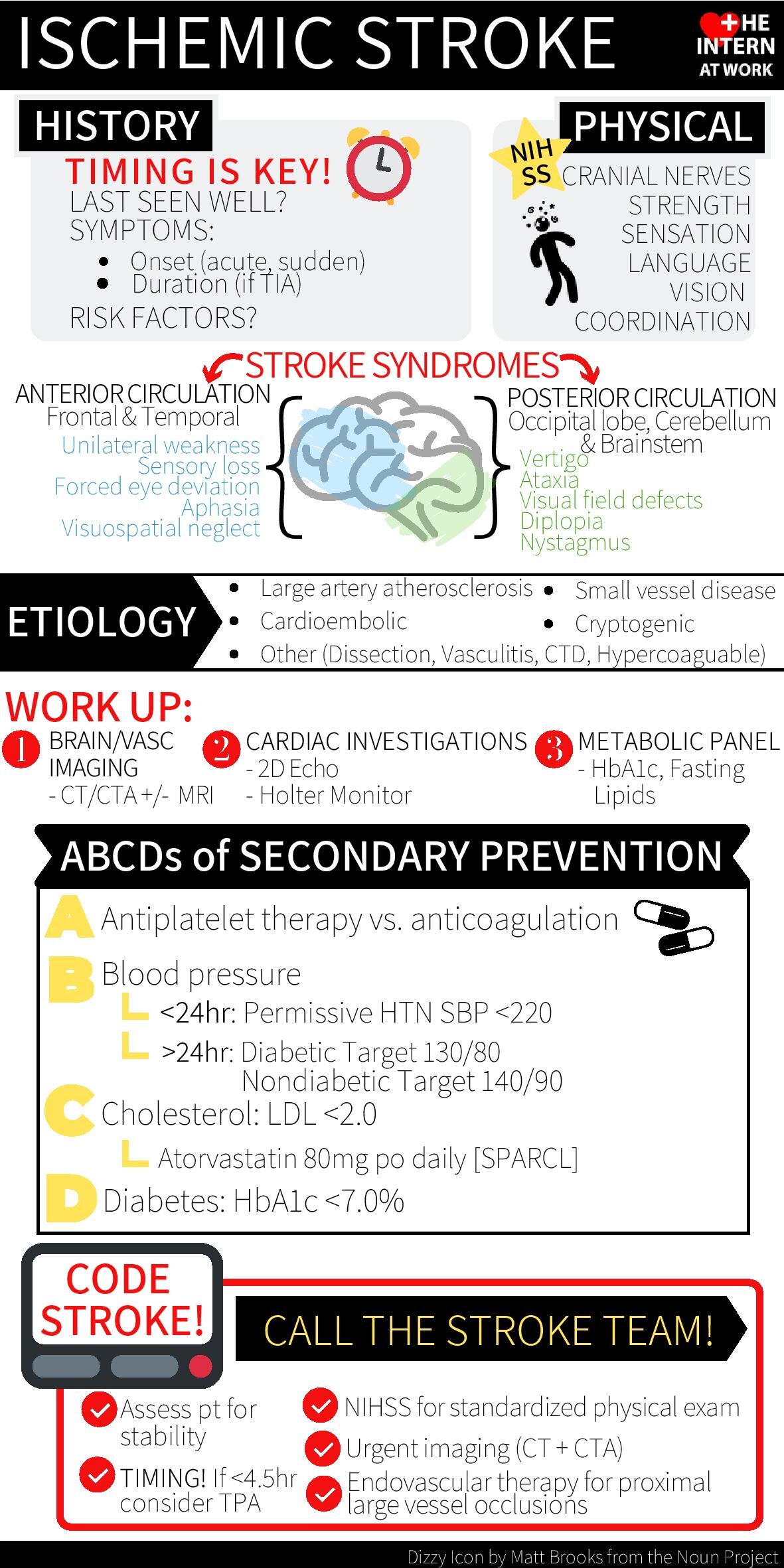
Ensure airway is protected, apply supplemental O2 if hypoxia & ensure adequate IV access
Physical examination to establish NIHSS score
History must establish timing of event, use collateral if needed to determine when patient last seen normal (LSN)
Acute Management of Ischemic Stroke Within The Window:
Contact local stroke team/telemedicine stroke neurologist
Obtain urgent CT/CTA “arch to vertex” to rule out hemorrhage and assess for embolism & extent of infarct
Check CBC, lytes, INR, PTT and glucose to assess for potential mimics of stroke & determine TPA eligibility
If patient is eligible for TPA ensure SBP <180mmHg and DBP<110mmHg (otherwise permissive HTN to SBP 220)
TPA should be considered in patients with LSN time of <4.5hrs and with no absolute contraindications
Eligibility time for EVT is evolving and decided in consultation with stroke team based on multiple clinical and imaging parameters
Non-Acute Management of Stroke:
Goal is to identify etiology of stroke and address modifiable risk factors
Investigations:
CT head
MRI if concerns for posterior fossa stroke
Assess for atrial fibrillation with Holter, +/- echocardiogram if cryptogenic
Carotic dopplers if CTA was not initially done
Check HbA1C & lipids
Management:
Antiplatelet agents (ASA + Clopidogrel) if no afib
ASA 81mg PO daily for all-comers
POINT trial recommends DAPT therapy for patients with high risk TIA and low risk strokes (NIHSS < 3) x 21 days, then Plavix 75mg PO daily alone
Anticoagulation if evidence of atrial fibrillation
Initiation of anticoagulation timing will depend on size of stroke and evidence of hemorrhagic transformation
BP control as per Hypertension Canada
Target: 140/90 mmHg
Target if patient is Diabetic: 130/80 mmHg
PROGRESS trial demonstrated use of ACE inhibitor + Thiazide Diuretic (Perindopril + Indapamide) decreased blood pressure and prevented stroke
Statin therapy to target LDL<2.0
SPARCL trial used Atorvastatin 80mg PO qhs and demonstrated decrease stroke recurrence in acute stroke.
Individualized diabetes therapy to target HbA1C <7.0%